CONSIDER CURRENT SCIENCE AROUND NADIR T SUPPRESSION LEVELS

Current science doesn’t just reflect T targets of <20 ng/dL, it also considers lowest T levels, also known as nadir T1
Evidence of nadir T level around prostate cancer treatments
Nadir serum testosterone or nadir T is the lowest value during androgen deprivation therapy (ADT)1
Sub-castrate testosterone nadir and clinical outcomes in intermediate or high-risk localized prostate cancer
Does degree of androgen suppression matter in hormone-sensitive prostate cancer?
Effectiveness of subcutaneously administered leuprolide acetate to achieve low nadir testosterone in prostate cancer patients
Nadir testosterone within first year of androgen-deprivation therapy (ADT) predicts for time to castration-resistant progression: a secondary analysis of the PR-7 trial of intermittent versus continuous ADT
Does nadir testosterone at the end of long term androgen deprivation therapy predict outcomes in high risk prostate cancer? Data from a phase Ill trial
Nadir testosterone after long-term followup predicts prognosis in patients with prostate cancer treated with combined androgen blockade
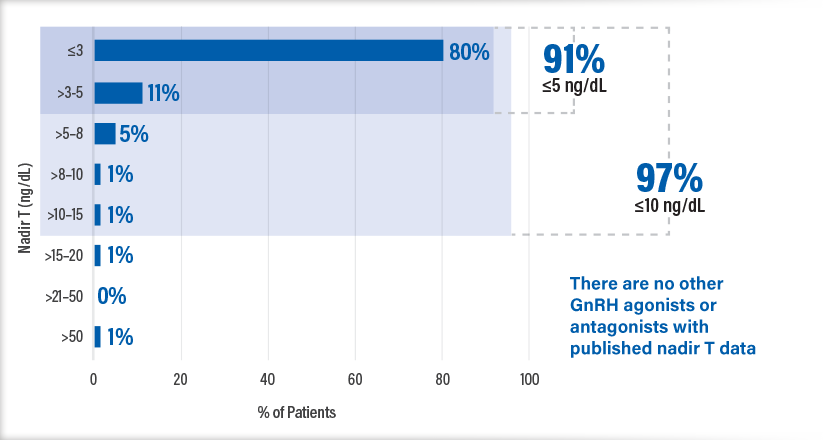
eligard ACHIEVED PROFOUND T SUPPRESSION ACROSS 1-, 3-, 4-, AND 6-MONTH DOSES7
The percentage of patients achieving serum testosterone concentration of ≤20 ng/dL across all studies*7
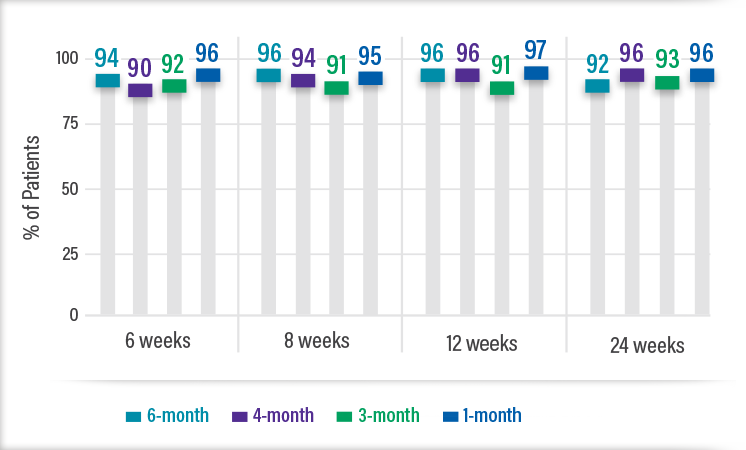
*Data from week 3 time point excluded as it reflects initial T surge and not final levels of suppression
Mean testosterone level (ng/dL) achieved across all doses at study conclusion8
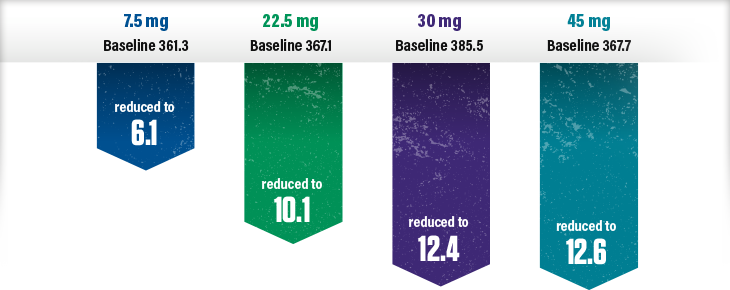
Achieving and maintaining low testosterone (T) to surgical castration level is the goal of ADT for advanced prostate cancer
Increasing evidence suggests that the historical target threshold for serum testosterone concentration when using ADT in treating advanced prostate cancer (≤50 ng/dL) is not equivalent to the concentrations achieved by surgical castration.“7
— Shore et al 2016Recommends 20 ng/dL for serum T during ADT in patients with advanced PCa as levels between 20 ng/dL and 50 ng/dL have worst clinical outcomes
Define target for T during ADT as <20 ng/dL
Encourages adoption of ≤20 ng/dL as castrate level. Recommends regular monitoring of T and PSA (3m–6m) as clinically appropriate during ADT and to reassess strategy if T not suppressed or PSA rises regardless of adequate T suppression
LOW OCCURENCE OF T MICROSURGES*1
Incidence of microsurges within 4 weeks after second dose
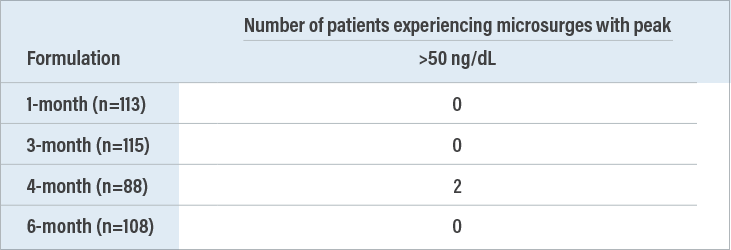
Pooled incidence of >50 microsurges was 2 out of 424 throughout the studies1
*Microsurge: absolute increase in T >25 ng/dL within 4 weeks after second dose
ELIGARD, a long-acting injectable, can help12
treatment
adherence
reliable and controlled T suppression
the possibility of T breakthroughs
eligard Helps achieve PSA goals
In all studies, ELIGARD decreased serum PSA in all patients whose baseline values were elevated above normal8
![]()
PSA levels are a good indicator of disease progression but measuring T levels ensures your patient continues to achieve the goal of ADT
|
|
For patients with metastatic prostate cancer, NCCN guidelines recommend ADT with treatment intensification, and ADT alone may be appropriate for some patients. This recommendation is based on the data showing improved survival in newly diagnosed patients with metastatic prostate cancer with a PSA value ≤4 ng/mL after 7 months of ADT. |